Introduction
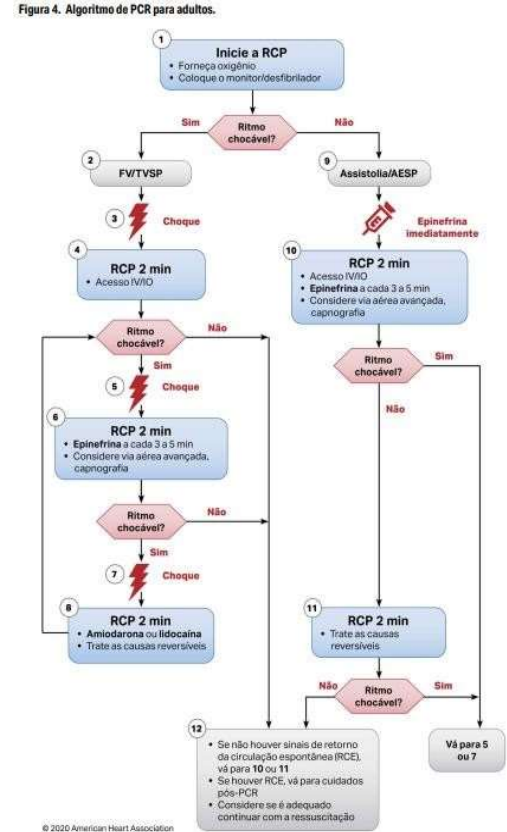
Advanced Cardiovascular Life Support (ACLS) goes beyond Basic Life Support (BLS). It includes the Secondary ABCD and post-cardiac arrest care. In this guide, we cover each step with essential clinical details for nursing and emergency medicine practice.
Advanced Airway (A)
Definitive airway is a priority. Options include endotracheal intubation (or orotracheal) and laryngeal mask airway (supraglottic). Prepare the equipment: laryngoscope, endotracheal tubes with stylet, bag-valve-mask with reservoir and oxygen, 20 ml syringe for cuff, stethoscope, tube holder, suction device and catheters.
Intubation should ideally be performed without interrupting chest compressions, aiming to complete within 10 seconds. Clinical confirmation includes bilateral chest expansion, auscultation over the epigastrium (no breath sounds) and bilateral lung fields. If selective intubation occurs, withdraw the tube 1 cm at a time, reassessing.
Capnography is recommended: ETCO2 < 10 mmHg indicates need to improve compressions; > 30 mmHg suggests return of spontaneous circulation (ROSC); 35-40 mmHg confirms correct tube placement.
Complications of Intubation
- Esophageal intubation.
- Selective intubation, lung collapse, and pneumothorax.
- Induction of vomiting and aspiration.
- Jaw dislocation.
- Soft tissue laceration (pharynx, epiglottis, larynx).
- Hemorrhage and aspiration.
- Tooth fracture or avulsion.
- Cervical spine injury.
Advantages of Advanced Airway
Maintains patent airway, allows suctioning of secretions, delivers high oxygen concentration, provides alternative route for drugs, and protects against aspiration.
Ventilation (B)
With advanced airway, ventilate at 10 breaths/min (1 every 6 seconds), without pausing compressions. Without advanced airway, maintain 30 compressions to 2 ventilations (100-120 compressions/min).
Beware of hyperventilation! It causes gastric distension, regurgitation, aspiration, increased intrathoracic pressure, reduced venous return, and decreased cardiac output.
Circulation (C)
Vascular access is a priority: 1st option: peripheral intravenous (IV) (drug reaches central circulation in 1-2 min); 2nd option: intraosseous (IO); 3rd option: endotracheal. After administering the drug, flush with 20 ml of saline and elevate the limb for 10-20 seconds.
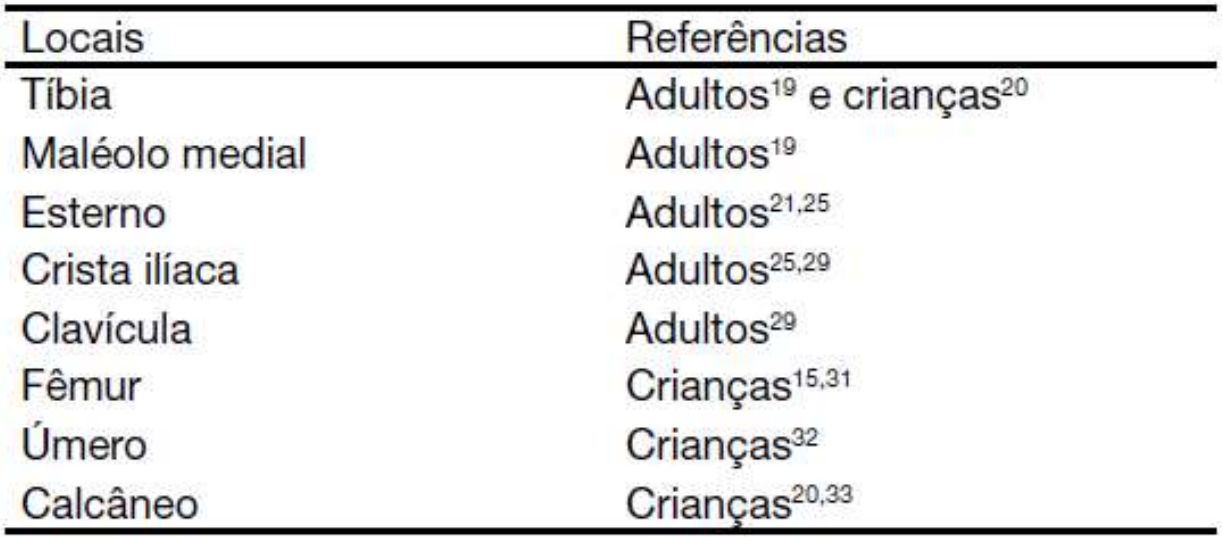
Intraosseous (IO) Access
Endotracheal Route
Use doses 2 to 2.5 times higher than IV, diluted in 5-10 ml of 0.9% saline or distilled water. Blood concentrations are lower than IV/IO. Absorbed drugs: ANEL – Atropine, Naloxone, Epinephrine, Lidocaine.
Conclusion
The secondary ABCD is the backbone of ACLS. Mastering airway, ventilation, and circulation saves lives. Practice with simulations and stay updated.