The Race Against Time in Chest Pain Care
A significant number of patients arrive at the emergency department with chest pain, but many do not receive adequate care. The initial approach should always be directed at confirming or ruling out the diagnosis of Acute Coronary Syndrome (ACS), especially Acute Myocardial Infarction (MI). Once MI is confirmed, emergency measures must be taken immediately to prevent complications, such as Heart Failure, and patient death.
Essential Nursing Interventions (NIC)
The nurse's role is crucial at every step. Key interventions include:
- Assess chest pain: intensity, location, radiation, duration, and precipitating and relieving factors.
- Obtain a 12-lead ECG within 10 minutes.
- Monitor neurological status, heart rhythm and rate.
- Choose the best lead for continuous monitoring (usually D2).
- Maintain a restful environment and administer medications for pain and ischemia relief.
- Evaluate medication effectiveness and auscultate heart sounds (presence of S3, intensity of heart sounds).
- Request chest X-ray, if appropriate.
Protocol Steps: Time is Muscle
The motto is clear: TIME = MUSCLE. The faster we act, the smaller the area of necrosis.
1. Patient Identification (Maximum 10 minutes)
Perform a rapid targeted assessment using the mnemonic MOVE:
- Monitoring (vital signs, oximetry, and ECG)
- Oxygen (if SpO2 < 90%)
- Vein (large-bore IV access)
- Exams (cardiac markers like Troponin, coagulation profile)
Additionally, obtain chest X-ray within 30 minutes and check contraindications for thrombolytics: active bleeding, coagulation disorders, previous hemorrhagic stroke, recent surgery/trauma, uncontrolled hypertension, pregnancy.
2. Care and Pain Relief: MONABICH
Pain relief is a priority. Follow the MONABICH protocol:
- Oxygen at 4 L/min if SpO2 < 90%
- Aspirin 160-325 mg (chew the tablet), if no contraindications
- Nitrate sublingual (Isordil® 5 mg every 3-5 min, up to 3 doses) – only if SBP > 90 mmHg and HR between 50-100 bpm. Do not use if suspected RV infarction or if phosphodiesterase inhibitors used in the last 24-48h.
- Morphine (2-4 mg IV) if pain persists after nitrate.
- Beta-blocker, ACE inhibitor, Clopidogrel, and Heparin.
Then, interpret the ECG to define specific management.
Pathology According to ECG
- ECG with ST elevation → STEMI: Provide immediate reperfusion. The choice between thrombolytic or angioplasty (PCI) depends on two criteria:
- Time since symptom onset:
- ≤ 12h: PCI (door-to-balloon time ≤ 90 min) or thrombolytic (door-to-needle time ≤ 30 min). Tenecteplase is first choice.
-
12h: Admission to ICU/CCU, observation, schedule catheterization.
- Infrastructure: Availability of coronary care unit for stenting.
- Time since symptom onset:
- ECG without ST elevation, but Troponin + → NSTEMI
- ECG without ST elevation and Troponin - → Unstable Angina (UA)
Thrombolytic Therapy vs. Angioplasty
Thrombolytic Therapy: Indicated when there is no time for angioplasty. Aims to dissolve clots and restore flow. Contraindicated in patients at risk of bleeding.
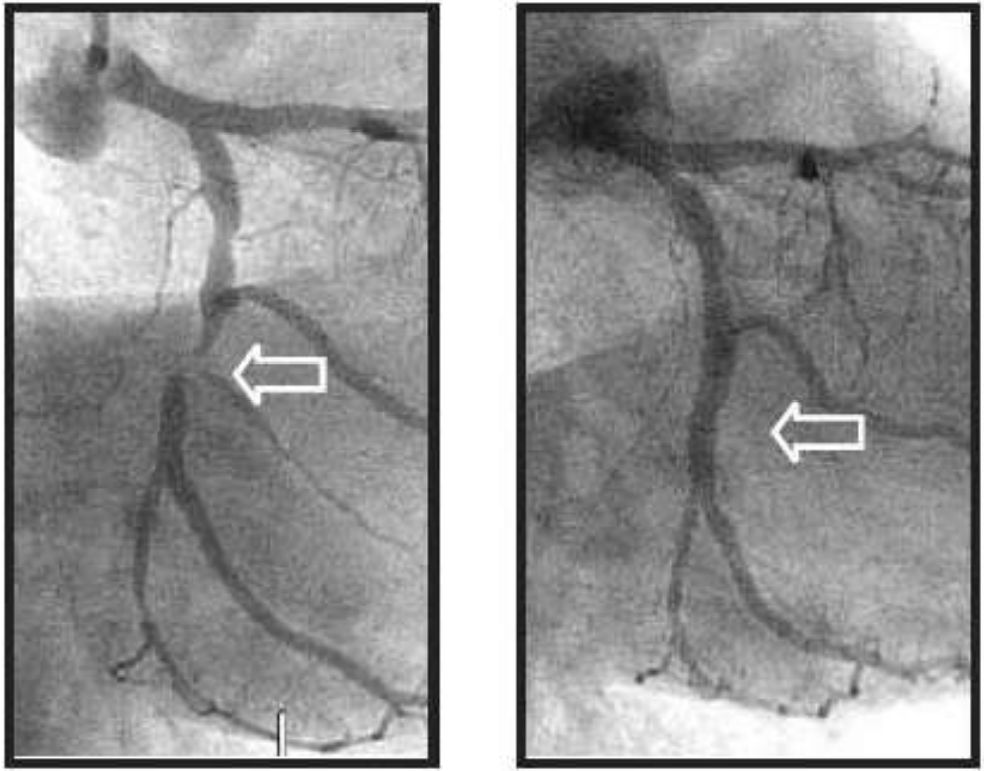
Percutaneous Coronary Intervention (PCI): Gold standard for MI treatment. Indicated for refractory anginal pain, partial (>70%) or total obstruction. Consists of artery stenting.
Revascularization (Bypass): Indicated for triple-vessel disease (stenosis >50% in all three main arteries) or left main coronary artery stenosis, with preserved ventricular function.
Post-MI Nursing Interventions (NIC)
- Identify and assess the patient with chest pain (Manchester Protocol, MOVE).
- Maintain rest and continuously monitor vital signs.
- Oxygen therapy if SpO2 <90%.
- ECG within <10 min, large-bore IV access.
- Administer protocol medications (MONABICH and/or thrombolytic).
- Reassess pain, control anxiety.
- Provide post-PCI care and implement the Nursing Process (data collection, nursing diagnoses, nursing prescriptions).
- Health education: guide on risk factors and lifestyle changes.
For further depth, watch the explanatory video: Chest Pain Protocol.