What is Ischemic Stroke?
Ischemic stroke (IS) occurs when there is an obstruction of a blood vessel that carries blood to the brain, resulting in sudden neurological deficit. It is the most common cause of stroke, accounting for 85-87% of cases. The term "stroke" is used for the lay public, but the correct medical nomenclature is Cerebrovascular Accident.
Only a minority of patients arrive at the emergency room in time to receive reperfusion therapy or hemorrhage control. This is due to the population's lack of knowledge about signs and symptoms, poorly structured health services, and absence of established protocols.
Types and Risk Factors
Ischemic stroke can be classified into:
- Large artery thrombotic: caused by atheromatous plaque.
- Small artery thrombotic: also called lacunar stroke.
- Cardiogenic embolic: resulting from atrial fibrillation (AF).
- Cryptogenic: without known etiology.
- Others: cocaine use, coagulopathies, contraceptives, arterial dissection.
Risk factors are divided into non-modifiable (age >55 years, female sex, black race, COVID-19, autoimmune diseases) and modifiable (hypertension, diabetes, obesity, high cholesterol, smoking, amphetamine use). About 80% of ischemic stroke cases are related to modifiable factors.
Pathophysiology and Sequelae
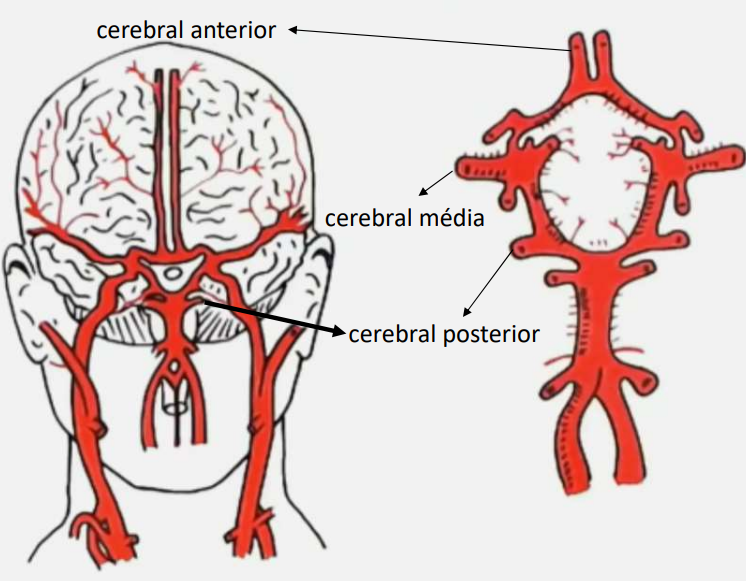
The brain consumes 20% of the oxygen supplied by circulation. Arterial obstruction leads to ischemia, hypoxia, anoxia, and necrosis of the ischemic core, with expansion of the penumbra zone and neuronal death. Common sequelae include:
- Motor function: hemiparesis and hemiplegia.
- Communication: apraxia and aphasia.
- Perception: hemianopsia.
- Sensory loss: changes in proprioception and interpretation of stimuli.
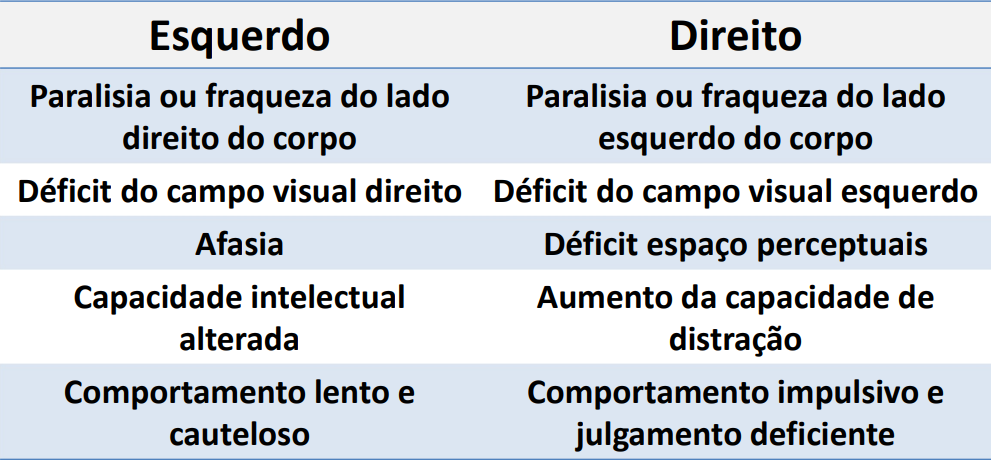
- Cognitive and psychological impairment: memory, learning, and behavior.
Warning Signs and Assessment Scales
Transient Ischemic Attack (TIA) is a temporary episode of neurological dysfunction lasting <1 hour, indicating a risk of ischemic stroke within the next 30 days (20-30% chance).
The Cincinnati Scale assesses three findings: facial droop, arm drift, and slurred speech. One positive finding confers 72% probability of ischemic stroke; three findings, >85%. In addition, use the Glasgow Coma Scale and the NIH Stroke Scale to assess neurological deficits and severity.
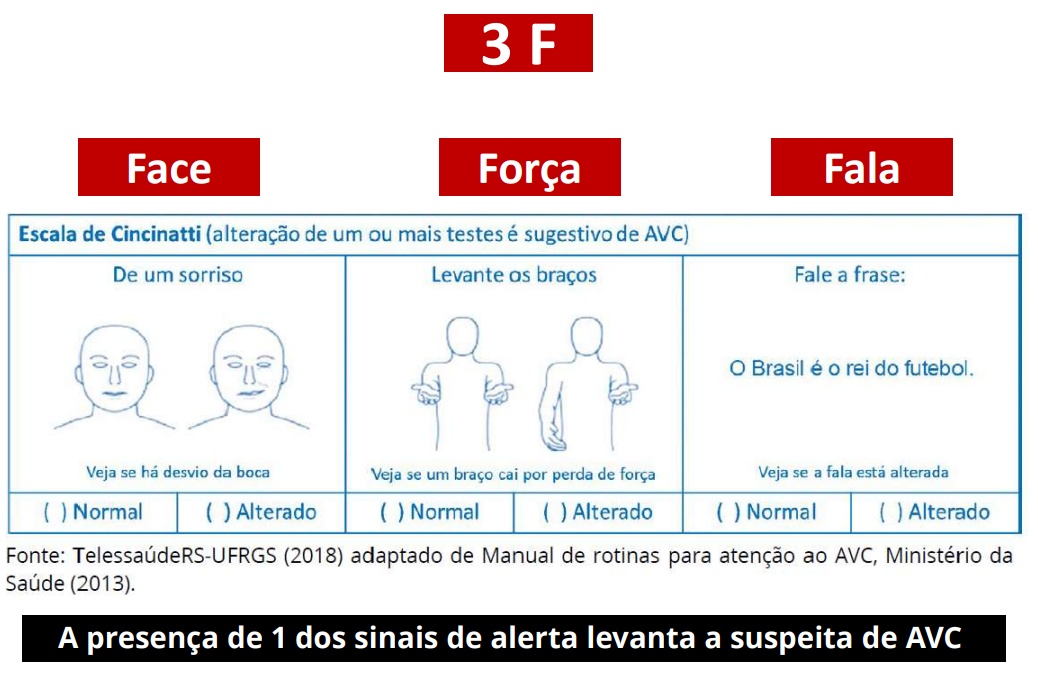
The "SAMU" 4F protocol (Face, Force, Speech, Phone) is a practical tool for rapid identification.

Nursing Process
The affected Basic Human Need (Wanda Horta) is Vascular Regulation. The priority nursing diagnosis is Risk for ineffective cerebral tissue perfusion, with risk factors such as aneurysm, atherosclerosis, AF, hypertension, among others.
NIC Interventions
- Promote cerebral perfusion: monitor hemodynamic parameters, position head of bed at 0-30°, administer thrombolytics per protocol.
- Monitor neurological status (Glasgow, Cincinnati, NIH).
- Control temperature (antipyretic if axillary >37.5°C).
- Oxygen at 4L/min if SpO2 <94%.
- Collect history and directed physical exam.
- Refer for head CT.
- Monitor blood glucose and ECG.
- Maintain cardiac monitoring.
- Prepare and administer thrombolytic therapy.
- Watch for signs of bleeding (risk of hemorrhagic transformation).
NOC Outcomes
Adequacy of cerebral blood flow to maintain brain function, with indicators such as SBP, DBP, ICP, fever, level of consciousness, and cognition.
Clinical and Imaging Diagnosis
Diagnosis is clinical, confirmed by head CT. In ischemic stroke, the image shows a hypodense area; in hemorrhagic stroke, a hyperdense area.
Treatment
The goal is to reduce sequelae and mortality. The time of symptom onset defines the approach:
- <4.5h: IV Thrombolytic Therapy with Alteplase (0.9 mg/kg, max 90 mg). Administer 10% in 1 minute and the remainder over 60 minutes. After, infuse 20 mL of 0.9% saline.
- >4.5h to 6h: Intra-arterial thrombolytic therapy.
- Up to 8h: Mechanical thrombectomy.
- >8h to 24h: Clinical treatment.
Exclusion Criteria for Thrombolytic Therapy
- Use of anticoagulants and altered coagulation.
- Severe TBI or ischemic stroke in the last 3 months.
- History of intracranial hemorrhage.
- Systolic BP ≥185 mmHg or diastolic BP ≥110 mmHg refractory.
- Mild neurological deficits.
- Major surgery in the last 14 days.
- Lumbar puncture in the last 7 days.
- Blood glucose <50 mg/dL with reversal after correction.
Post-Thrombolysis Care
- Neurological assessment (NIHSS) every 5 minutes during infusion, every 15 minutes for the first 2 hours, every 30 minutes for the next 6 hours, and every 1 hour until 24 hours.
- Do not perform arterial puncture or central venous catheter in the first 24h.
- Do not insert urinary catheter until 30 minutes after infusion ends.
- Do not insert nasogastric tube in the first 24h.
- Monitor BP strictly (SBP <185, DBP <110 mmHg).
- Do not use antithrombotics in the first 24h.
Complications
The main complication is hemorrhagic transformation. Suspect if there is worsening of neurological deficit, sudden headache, nausea, or vomiting. In this case, discontinue rt-PA, request urgent head CT, and neurosurgical evaluation.
Sequelae and Impacts
Common sequelae include cognitive, communication, motor, swallowing impairment, and incontinence. They can lead to aspiration pneumonia, urinary infections, malnutrition, dehydration, DVT, PE, and pressure ulcers.
Complementary Video
Watch the video on diagnosis and treatment of ischemic stroke: https://www.youtube.com/watch?v=djDMNLH0D_I