The Challenge of Major Burns
Burns are skin injuries caused by thermal, chemical, or electrical agents that generate excessive heat, leading to cell death. They may require emergency hospital treatment and, in severe cases, can be fatal. The clinical relevance goes beyond the immediate injury: functional, aesthetic, and psychological sequelae profoundly impact quality of life.
The extremes of age (elderly and children) and people in labor activities are the most affected. Ideally, treatment should occur in a Burn Referral Center — in Belo Horizonte, Hospital João XXIII is the reference.
Classification of Burns
By Type/Etiology
- Thermal: Result from energy transfer from a heat source to the body. They can be caused by dry or moist heat (hot water, steam, fire).
- Electrical: Caused by electrical discharges (burns similar to thermal) or by direct passage of electrical current through the body. They present an entry and exit point.
- Chemical: Caused by acids or bases that, when absorbed, can damage internal organs. The degree of destruction depends on the nature, concentration, and duration of contact.
- Radiation and Inhalation: Include sunburns and injuries from smoke or steam inhalation.
By Depth
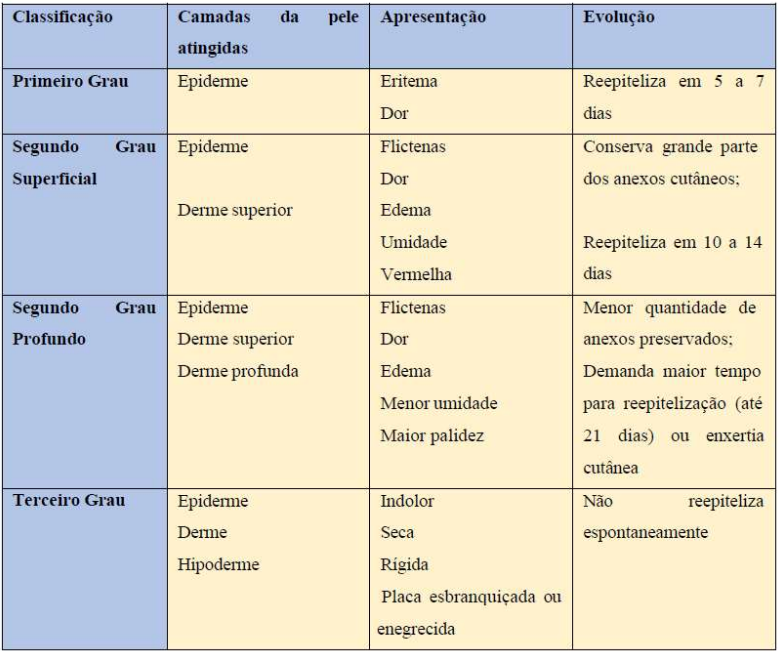
- 1st Degree – Superficial: Destruction of only the epidermis. Presence of erythema, blanches under pressure, and is painful.

- 2nd Degree – Partial Thickness: Destruction of total epidermis and partial dermis. Exudative, erythematous, painful, with presence of blisters.

- 3rd Degree – Full Thickness: Destruction of total epidermis and dermis. Dry, hard, inelastic, translucent lesion, with visible thrombosed vessels. Painless to local puncture.

By Extent (TBSA)
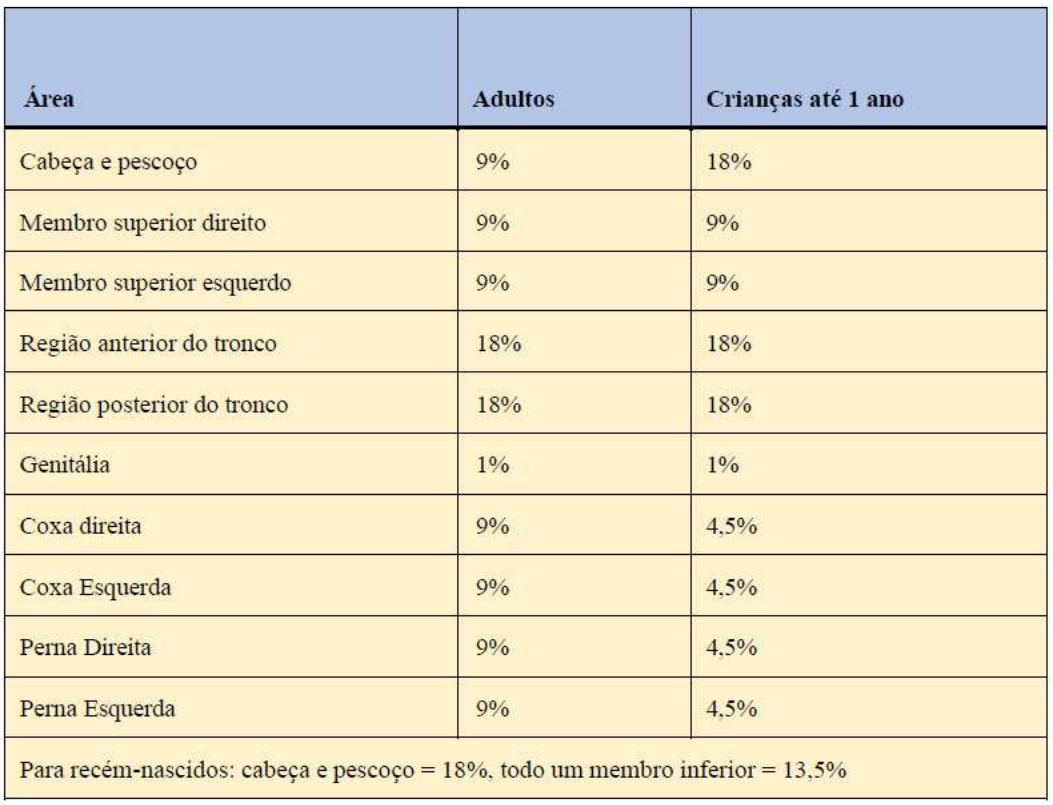
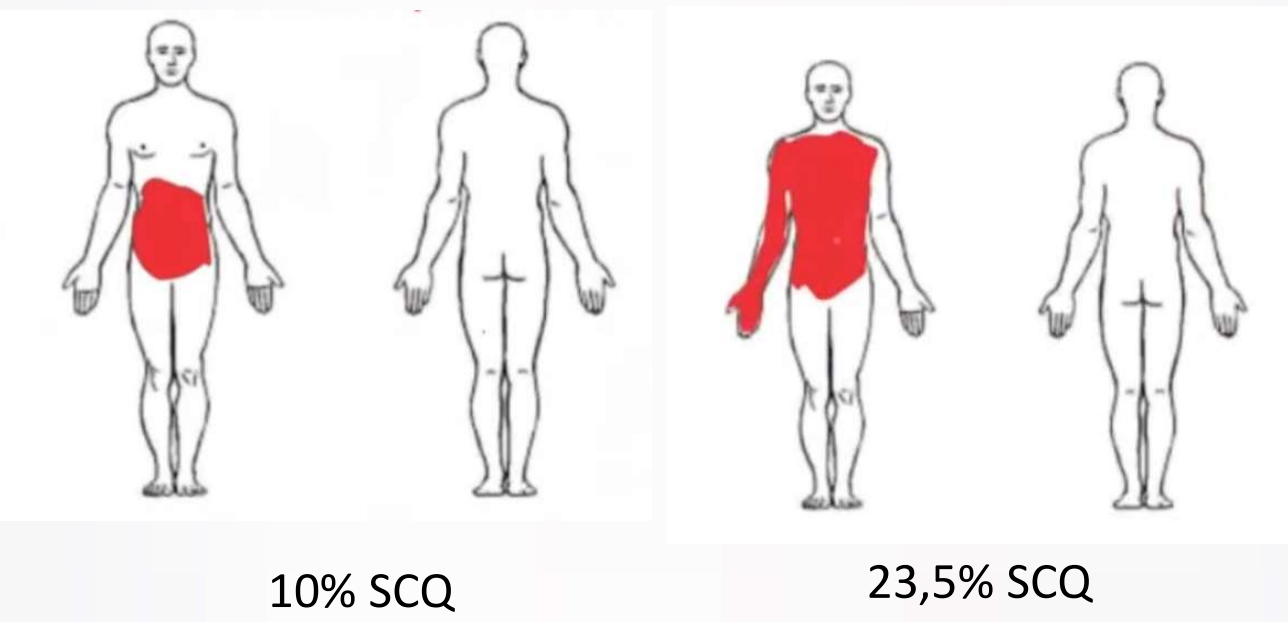
The Total Body Surface Area (TBSA) burned is calculated using the Rule of Nines or the Lund and Browder Chart.
Rule of Nines by Pulaski and Tennyson:
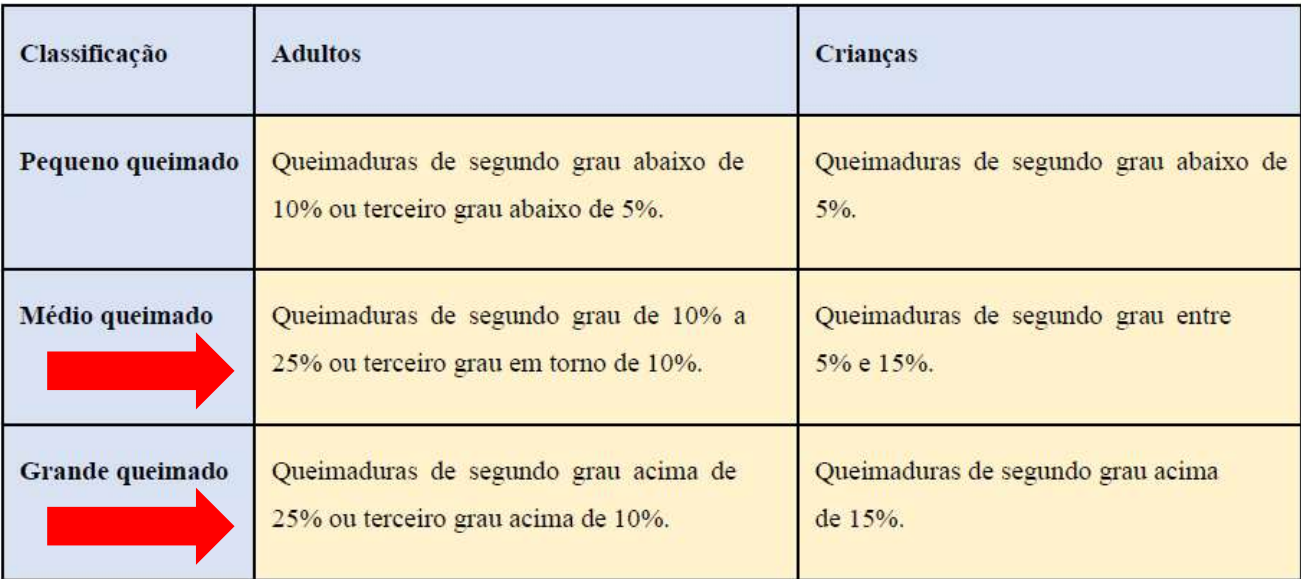
Classification by Extent:
Generally, the individual's palm represents 1% of body surface area, useful for estimating extent.
XABCDE-F of Major Burns
Management follows the XABCDE protocol, with the addition of F — Fluid therapy (volume resuscitation).
- Volume Resuscitation: Calculated with 2ml Ringer's Lactate x kg x TBSA (adults) and 3ml RL x kg x TBSA (children < 14 years). In children < 30 kg, add maintenance glucose solution. In electrical injuries, use 4ml RL x kg x TBSA until urine clears.
- Administration: Half the volume (50%) in the first 8 hours after the event, and the remainder over the next 16 hours.
Management of Minor Burns (Stable Patients)
- IV analgesia, if necessary.
- Cleaning of areas with 2% chlorhexidine scrub and 0.9% saline.
- Debridement of devitalized tissue and rupture of blisters.
- Dressing with 1% silver sulfadiazine (abundant), occluded with gauze and crepe bandage.
- Referral to Burn Outpatient Clinic (mild cases) or Primary Health Unit.
- 1st degree burns: do not use occlusive dressings or special ointments; advise hydration with creams or oils.
Management of Moderate and Major Burns
- Perform ABCDEF and MOVE: Monitor vital signs, diuresis (CVC with UO of 0.5 to 1 ml/kg/hour) and analgesia; Oxygen; Vein (2 IV lines for resuscitation); Exams per protocol.
- Assess inhalation injury: cervical/facial burns, soot in eyelashes/nasal hairs, carbonaceous sputum, hoarseness, confusion, carboxyhemoglobin > 10%.
- Orotracheal intubation if: stridor, progressive hoarseness, use of accessory muscles, marked facial/neck edema, decreased level of consciousness, hypoxemia, hypercarbia.
- Elevate head of bed to 45° and affected limbs.
- Assess and record: TBSA, depth, causative agent, time elapsed, medications/fluids administered.
- Debridement under analgesia or anesthesia.
- Hair removal in burned areas.
- Do not use systemic antibiotics in the initial phase; use 1% silver sulfadiazine topically and occlusive dressing.
- Avoid succinylcholine (risk of hyperkalemia).
Escharotomy is indicated in 3rd degree burns with rigid circumferential eschars on limbs or chest plates with respiratory restriction.
- Chest: incision in anterior axillary line joined to line below the last costal arches.
- Limbs: medial and lateral incisions.
Complementary exams: CBC, coagulation panel, electrolyte panel, BUN/creatinine, glucose, blood gas, albumin, lactate, ECG, urinalysis, chest X-ray, CK, blood cultures (if infection suspected).
In-Hospital Monitoring
- Daily assessment of vital signs, fluid balance (UO) – risk of shock and acute kidney injury (30% of cases).
- Start thromboprophylaxis for DVT/PE.
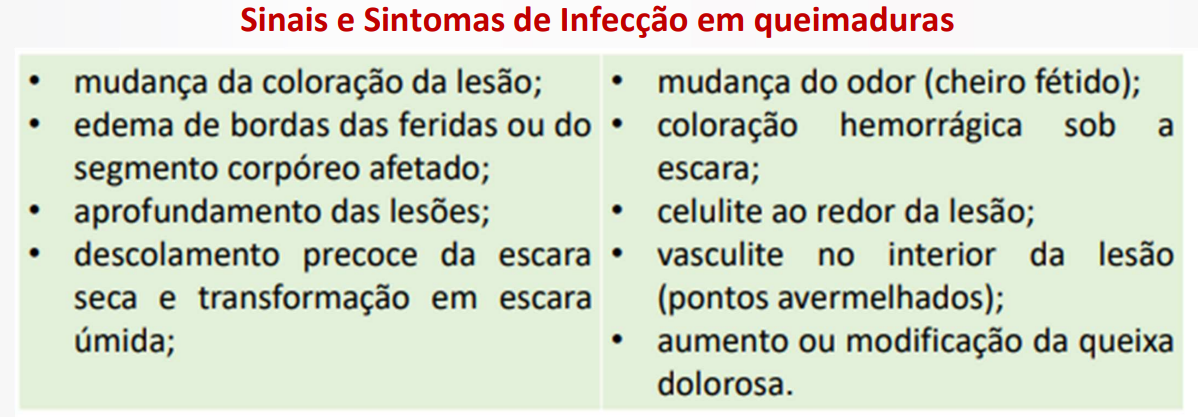
- Assess wound evolution and prevent infection/sepsis.
Nursing Diagnoses, Outcomes, and Interventions
Impaired Skin Integrity (Priority)
- Goal: Restore skin integrity.
- Interventions:
- Assess wound appearance and perform dressing.
- Observe signs of infection.
- Reposition every 2 hours.
- Position for optimal circulatory flow.
- In the first 30 minutes, use compresses with room temperature water (20-25°C) to limit extent and relieve pain.
- Clean with chlorhexidine.
- Irrigate with 0.9% saline.
- Debride loose skin and fragile blisters.
- Apply 1% silver sulfadiazine.
Deficient Fluid Volume (Priority)
- Goal: Adequate hydration.
- Interventions:
- Obtain central venous access (preferred in instability).
- Volume resuscitation using Parkland formula.
- Bladder catheterization: expected UO in adults 0.5-1 ml/kg/h, children 1.5 ml/kg/h.
- Monitor urine output.
- Perform fluid balance and electrolyte control.
- Monitor vital signs.
Risk for Infection
- Goal: Control of risks.
- Interventions:
- Hand washing before and after procedures.
- Assess patency of venous access.
- Watch for signs of inflammation at insertion sites.
- Aseptic technique.
- Diet rich in iron, zinc, and vitamin C.
- IV antibiotic prophylaxis in major debridements, grafting, or suspected infection.
Other Diagnoses
- Acute Pain – do not neglect!
- Ineffective Breathing Pattern
- Impaired Gas Exchange
- Risk for Shock
Exercise
(Municipality of Vitória-ES/AOCP/2019) Patient 30 years old, 70 kg, 2nd degree burn on entire right upper limb (hand, forearm, and anterior and posterior arm) and anterior region of face and neck. Estimated TBSA: 13.5%. Minimum volume in first 8h: 945 mL (option c).