What is Mechanical Ventilation?
Mechanical ventilation (MV) is a method of support for the treatment of Acute or Acute-on-Chronic Respiratory Failure, using positive pressure to assist or replace spontaneous ventilation. Understanding its fundamentals is essential for nurses, physiotherapists, and physicians working in intensive care units.
Ventilatory Support: Objectives and Modalities
The main objective of ventilatory support is to improve gas exchange, reduce respiratory work and effort, and decrease oxygen consumption. It can be performed Non-Invasively (NIV) or Invasively.
Non-Invasive Ventilation (NIV)
NIV is indicated for patients with minute volume > 4 L/min, PaCO2 < 50 mmHg, and pH > 7.25 (acidemia or acidosis). Its goal is to prevent progression to muscle fatigue and/or respiratory arrest. The main determinants are:
- Inspiratory Pressure (IPAP or PSV)
- Expiratory Pressure (EPAP or PEEP)
- CPAP: Continuous Positive Expiratory Pressure
Common devices include ETT, nasotracheal tube, tracheostomy tube, and laryngeal mask.
Invasive Ventilation
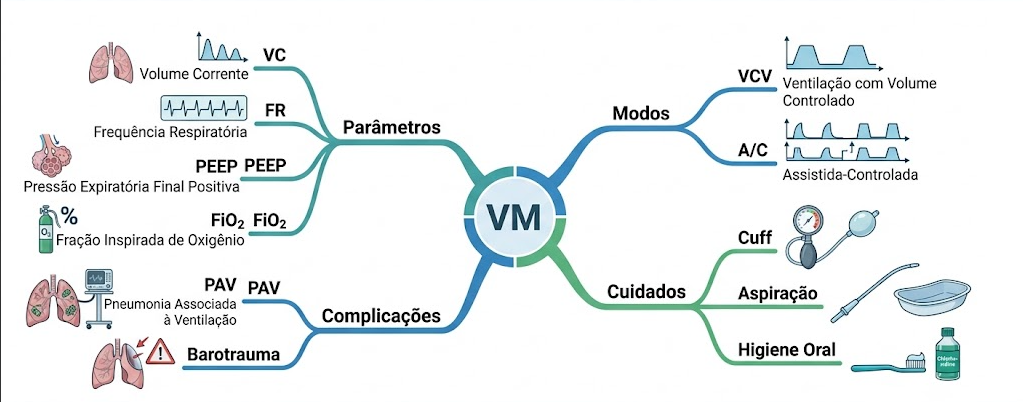
In invasive ventilation, parameters must be adjusted precisely:
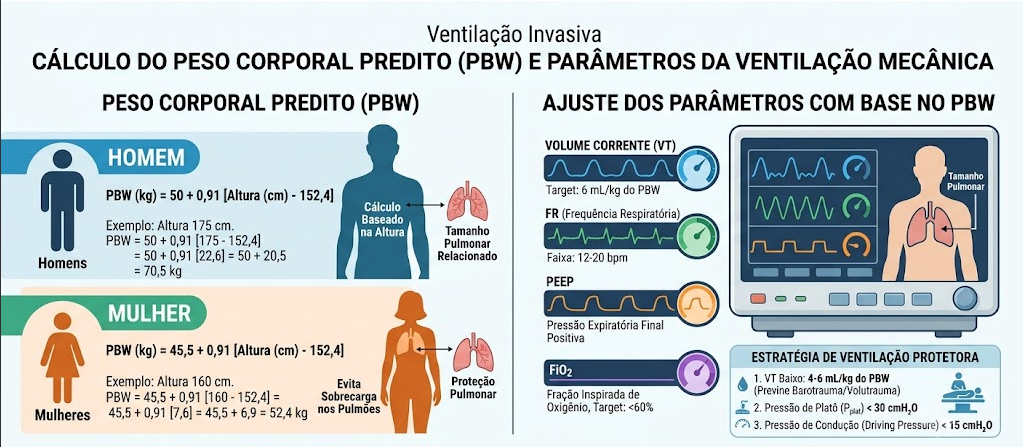
- Tidal Volume (VT): 6 ml/kg, using Predicted Body Weight (PBW)
- Men: 50 + 0.91 × (height in cm – 152.4)
- Women: 45.5 + 0.91 × (height in cm – 152.4)
- Respiratory Rate (RR): 12-16 breaths/min
- Inspiratory/Expiratory Ratio (I:E): 1:2 or 1:3
- Sensitivity: usually 2 L/min (for A/C mode)
- PEEP: adjusted in combination with FiO2 to maintain alveolar perfusion (5-10 cmH2O)
Important notes:
- Maintain continuous pulse oximetry
- Perform blood gas analysis 30 minutes after MV initiation
- Assess hemodynamic repercussions, especially in patients with heart failure or acute pulmonary edema
- Asynchrony can occur in 10-80% of patients, especially when ventilator sensitivity is inadequate and the patient has respiratory drive
Essential Concepts: Ventilation, Oxygenation, and Perfusion
Ventilation is different from oxygenation, which is different from perfusion. Each concept involves a different diagnosis, and the clinical picture combined with blood gas analysis will dictate the scenario.
- Compliance: elastic force/alveolar tension, directly corresponds to the maximum volume/pressure of the alveolus.
- Resistance: dictated by pressure/airflow.
Nursing Diagnoses (NANDA) and Interventions (NIC)
Impaired Spontaneous Ventilation
Expected Outcome (NOC): Respiratory Status: Ventilation
Nursing Interventions (NIC):
- Ventilatory assistance
- Oxygen therapy
- Respiratory monitoring
- Mechanical Ventilation Management: Invasive
- Assemble the circuit with inspiratory and expiratory limbs and monitoring cables
- Check connections to ensure they are secure
- Configure the device – physician and physiotherapist
- Turn on alarms
- Educate the patient and family
- Assess need for sedation and neuromuscular blockers (collaborative)
- Monitor MV effectiveness (blood gas analysis) on physiological and psychological status whenever adjustments are made
- Provide alternative means of communication
- Drain condensed water from the circuit
- Document MV settings and changes
- Monitor adverse effects: tracheal deviation, infection, barotrauma, volutrauma, reduced cardiac output, gastric distension, subcutaneous emphysema
- Monitor for detection of oral, nasal, tracheal, laryngeal injury – artificial airway and fixations
- Position in bed for good ventilation/perfusion (good lung down) – discuss with team (Fowler or Semi-Fowler, RLD or LLD?)
Ineffective Airway Clearance
Expected Outcome (NOC): Respiratory status: airway patency
Nursing Interventions (NIC):
- Artificial airway management
- Change to oropharyngeal airway – if biting on ETT
- Humidification/heating of gases
- Maintain good systemic/oral hydration
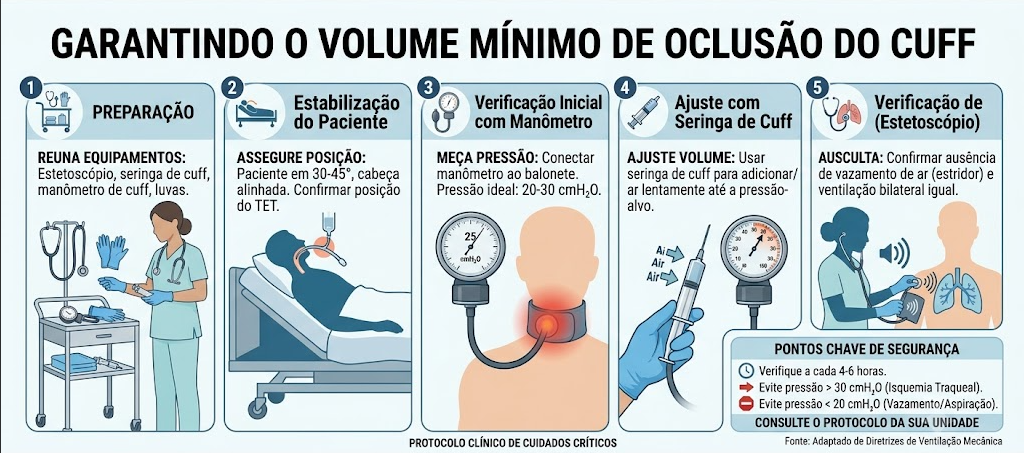
- Keep cuff inflated at 15 to 25 mmHg
- Monitor cuff pressure every 4-8h
- Auscultate chest after each ETT manipulation
- Check internal pressure with cuff manometer whenever patient is repositioned
- Observe the rim and maintain its positioning
- Keep the MV circuit in constant support, avoiding traction
- Ensure ETT safety during position changes, oral hygiene, suctioning
- Perform tracheal suctioning if necessary
- Record secretion characteristics
- Oral care: hygiene, suctioning, hydration
- Monitor MV pressures and volumes (increased inspiratory pressure and decreased expiratory volume)
- Keep manual resuscitation bag assembled at bedside
- Head of bed elevated
- Tracheostomy – hygiene, dressing
- Inspect peristomal skin: drainage, erythema, irritation, bleeding
- Palpate for subcutaneous emphysema
- Change fixation daily or as needed
Ventilatory Modes
- VCV (Volume-Cycled Ventilation): Predetermined VT – caution with barotrauma and pneumothorax. Inspiratory pressure is limited by the ventilator.
- A/C (PCV): Variable VT, as the patient determines movements and the ventilator maintains positive end-expiratory pressure (PEEP).
Relevant Aspects in Practice
- Check and record programmed and delivered MV parameters
- Ensure continuous pulse oximetry
- Install capnograph if possible
- Collect blood gas ~20 min after any adjustment or when clinical status changes, and once daily in the acute phase
Prevention of Ventilator-Associated Pneumonia (VAP)
VAP can occur generally 48h after intubation. Preventive measures include:
- Change circuit if soiled (e.g., blood, vomit) or damaged
- Change humidifiers every 7 days
- Use cuffed tubes to prevent aspiration
- Cuff pressure – minimum 25 cmH2O (depending on reference)
- Head of bed elevated 30 to 45°
- Oral hygiene with 0.12% chlorhexidine mouthwash
- Daily sedation interruption
Ensuring Minimal Occlusive Volume
- Suction oral cavity
- Position stethoscope laterally to the trachea
- Inflate the cuff and auscultate for sounds of air passing
- Stop inflation when sounds cease
- Remove 0.5 ml (from syringe) until you hear the sound of air passing again
- Reinflate SLOWLY until the sound ceases again
- Check pressure with cuff manometer
- Record
Respiratory Failure
Inability of the lungs to efficiently perform gas exchange to maintain aerobic metabolism and CO2 excretion.
Can lead to Hypoxemia (ARDS, PE) and/or Hypercapnia (COPD – Asthma, Bronchitis, Emphysema).