The Heart in Danger: Understanding Infarction
Acute Myocardial Infarction (AMI) is a medical emergency that requires fast and precise action. As an emergency nurse, I know that every minute counts to save the heart muscle. Let's dive into the details that make a difference in clinical practice.
Coronary Artery Disease (CAD) is the main cause of AMI. It manifests in two forms: stable angina (pain on exertion, with occlusion <70%) and unstable angina (pain at rest, occlusion >70%). Both are partial occlusions, but unstable angina already signals imminent risk of infarction.
In the acute form of CAD, we have AMI or Acute Coronary Syndrome (ACS). In the chronic form, systemic changes such as Heart Failure are more common. AMI is further subdivided into ST-segment elevation MI (STEMI, necrosis) and non-ST-segment elevation MI (NSTEMI, ischemia).
Anatomy and Pathophysiology: Where It All Begins
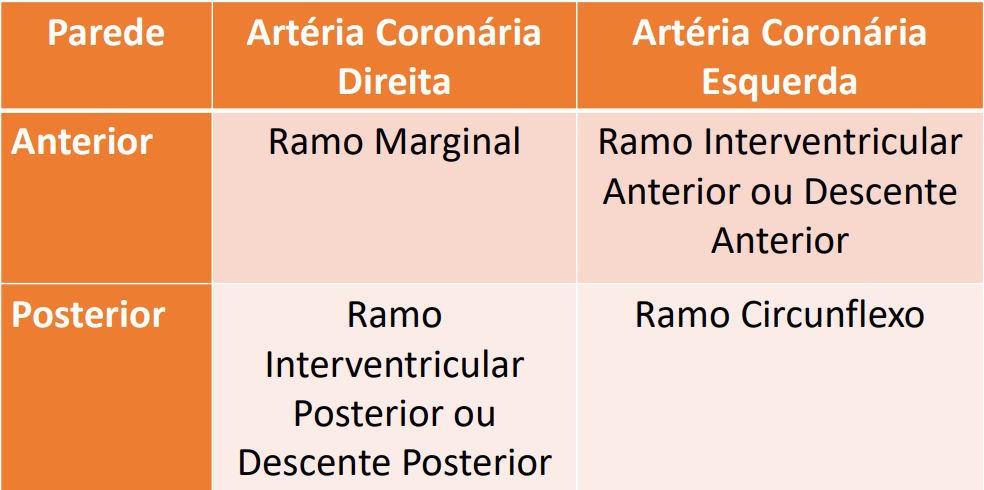
The image above shows the affected arterial walls (anterior or posterior) and the regions of the heart supplied by the right and left coronary arteries. The accumulation of LDL in the tunica intima, driven by risk factors such as smoking and a high-fat diet, leads to the formation of atherosclerotic plaque.
The inflammatory process creates a fibrous cap around the lipid. When this plaque ruptures, a thrombus forms. Total occlusion by the plaque causes STEMI; partial occlusion by the thrombus leads to NSTEMI; and partial occlusion by the plaque results in unstable angina.
Risk Factors: Know to Prevent
Non-modifiable: age (men >55, women >65) and family history of CAD in a first-degree relative.
Modifiable: hyperlipidemia, smoking, hypertension, obesity, sedentary lifestyle, diabetes mellitus, metabolic syndrome, and cocaine/amphetamine use. These factors act silently, and 50% of men and 64% of women who die suddenly from AMI had no prior symptoms.
Clinical Manifestations: The Pain That Alerts
Chest pain is the classic symptom. In stable angina, it ceases with rest or nitrates. In unstable angina and AMI, the pain is persistent and does not improve with medication. Always investigate location, radiation, and aggravating/relieving factors.
Attention: elderly, women, diabetics, chronic kidney disease patients, and those with dementia may not present typical pain. Be alert for ischemic equivalents: dyspnea, nausea/vomiting, malaise, palpitations, syncope, and confusion.
Physical Examination: Warning Signs
Physical exam is usually normal, but some findings indicate poor prognosis: systolic murmur at the mitral focus, third heart sound, tachycardia, tachypnea, hypotension, diaphoresis, weak pulses, and pulmonary crackles. These signs suggest severe ventricular dysfunction.
Diagnosis: Confirming AMI
Diagnosis combines clinical presentation, electrocardiogram (ECG), troponin levels (first-choice biomarker), and cardiac catheterization (gold standard).
On ECG, ST elevation indicates recent necrosis; Q wave indicates old infarction. ST depression suggests ischemia; T wave inversion also points to ischemia. Troponin begins to rise 3 hours after symptom onset, peaks at 18-24 hours, and lasts up to 10 days.
Diagnostic summary:
- Unstable angina: ischemic symptoms, normal ECG and enzymes.
- NSTEMI: symptoms, no ST elevation on ECG, elevated troponin.
- STEMI: symptoms, ST elevation on ECG, elevated troponin.
Nursing Care: Diagnoses and Interventions
The main Nursing Diagnoses in AMI include:
- Acute pain related to myocardial ischemia.
- Risk for decreased cardiac tissue perfusion due to factors such as drug abuse, DM, HTN, hyperlipidemia, family history, etc.
- Risk for impaired gas exchange.
- Anxiety related to the acute condition.
- Deficient knowledge about risk factors and self-care.
Strictly follow the Chest Pain Protocol to ensure a rapid and effective approach. Continuous monitoring, administration of oxygen, nitrates, and analgesia, as well as emotional support, are pillars of care.
Remember: AMI is a race against time. Your knowledge and agility can make all the difference between life and death. Stay updated and confident in clinical practice.