What is Polytrauma?
The polytrauma patient is one who has suffered multiple traumas, often with injuries to more than one system or region of the body. The care of these victims requires a rapid, organized approach based on well-established protocols.
Essential Aspects of Care
The key to success lies in the rapid identification of injuries, always remembering the biomechanics of trauma to anticipate possible damage. Immediate therapeutic intervention and control of life-threatening conditions — such as hemorrhages and airway obstruction — are absolute priorities, following the famous XABCDE-F.
It is essential to analyze the number of victims and available resources. When there is more than one victim, prioritization should be:
- Risk of death
- Risk of limb loss
- Other risks that do not threaten life or limbs
Identify victims with the greatest chance of survival using the START (Simple Triage And Rapid Treatment) method, which takes 30 to 60 seconds per victim.
START Triage System
START classifies victims into four categories:
- Red → Immediate Care! Patients with critical injuries that require minimal time or equipment for treatment and have a good prognosis if treated quickly. Examples: compromised airway, external hemorrhage.
- Yellow → Can Wait! Serious injuries, but that do not require immediate care to preserve life or limb. Example: long bone fracture.
- Green → Can Walk! Injured who ambulate, with minor injuries, who can wait for treatment or even help with transport.
- Black → Very Serious and/or Dead! Injuries so severe that the chance of survival is minimal or nil. Example: patients in cardiorespiratory arrest.
XABCDE-F: The Primary Assessment
The XABCDE-F should be performed in 2 to 5 minutes, without exceeding 10 minutes at the accident scene. Remember to treat conditions as you find them. Transport to the referral hospital should be as quick as possible.
X – Hemorrhage Control
The primary assessment only progresses after hemorrhage control. Use tourniquet, hemostatic agent (kaolin or chitosan) or direct compression (manual for 10 minutes or compressive dressing). According to PHTLS, there is no insignificant bleeding; every red blood cell counts.
A – Airway and Cervical Spine
Start with manual immobilization and careful alignment of the head in neutral position. Check the patient's ability to speak — ask: "What is your name? What happened?"
Inspect the oral cavity for obstruction by:
- Tongue fall
- Vomitus, blood, or foreign body
- Bucomaxillofacial trauma
- Extensive facial burn
Clear the airway with:
- Head Tilt, Chin Lift or Jaw Thrust
- Suction (preferably with rigid catheter)
- Oropharyngeal airway (Guedel) or nasopharyngeal in unconscious patients — beware of intact gag reflex
- O₂ administration (non-rebreather mask)
- Tracheal intubation (orotracheal or nasotracheal) in severe TBI with decreased level of consciousness
- Cricothyroidotomy in facial trauma with severe mandibular and maxillary fractures
Cervical collar and rigid backboard should be maintained until exclusion of fracture or ligamentous injury of the cervical spine. Use the backboard for transport until hospital radiological study.
B – Breathing
Assess the pattern and quality of breathing. The respiratory rate (RR) can be:
- Absent → apnea
- Slow → bradypnea (< 10 breaths/min)
- Normal → 10-12 to 20 breaths/min
- Fast → tachypnea (20 to 30 breaths/min)
- Very fast → > 30 breaths/min
Provide the highest possible flow (10-15 L/min) during the primary exam.
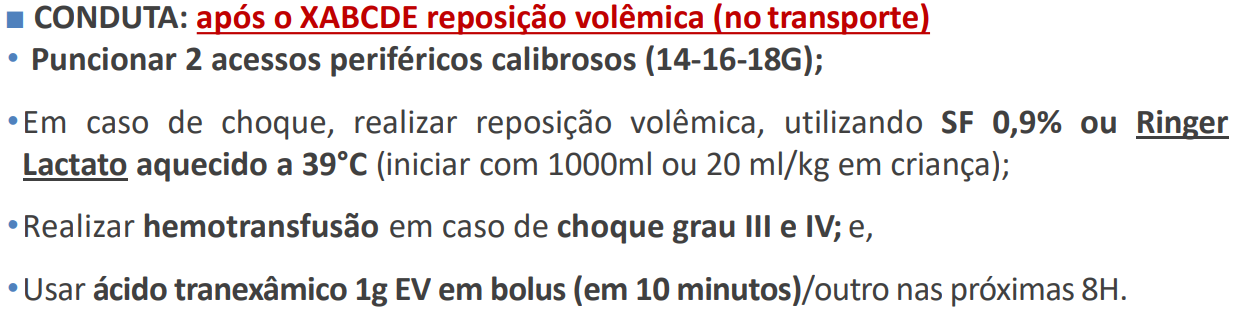
C – Circulation and Signs of Shock
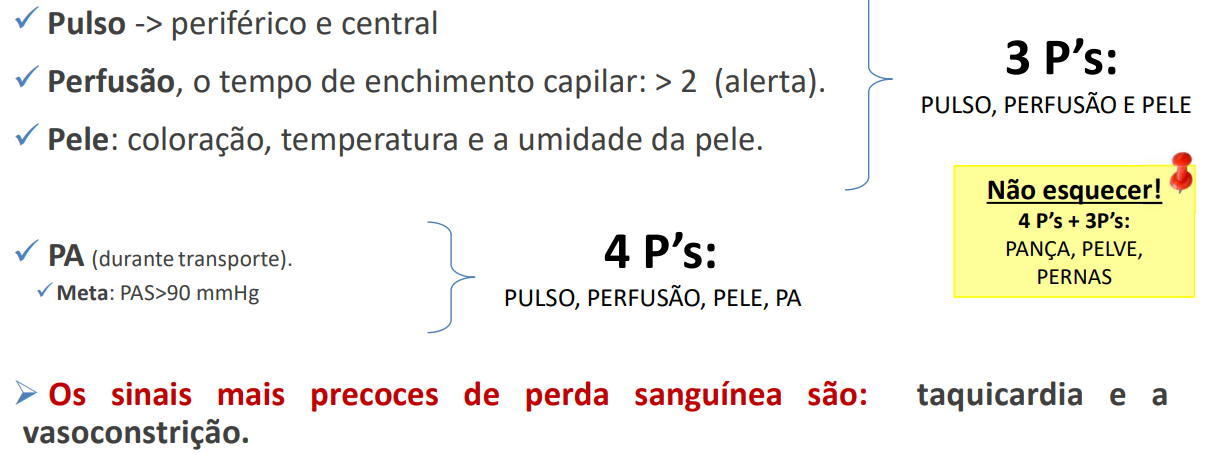
Every trauma patient with tachycardia, cold/clammy/pale/cyanotic skin and capillary refill ≥ 3 seconds is in hemorrhagic/hypovolemic shock until proven otherwise. Do not waste time at the scene.
D – Neurological Status
TBI classification by Glasgow Coma Scale (GCS):
- Mild: GCS 13-15
- Moderate: GCS 9-12
- Severe: GCS 3-8 (requires intubation and intensive care)
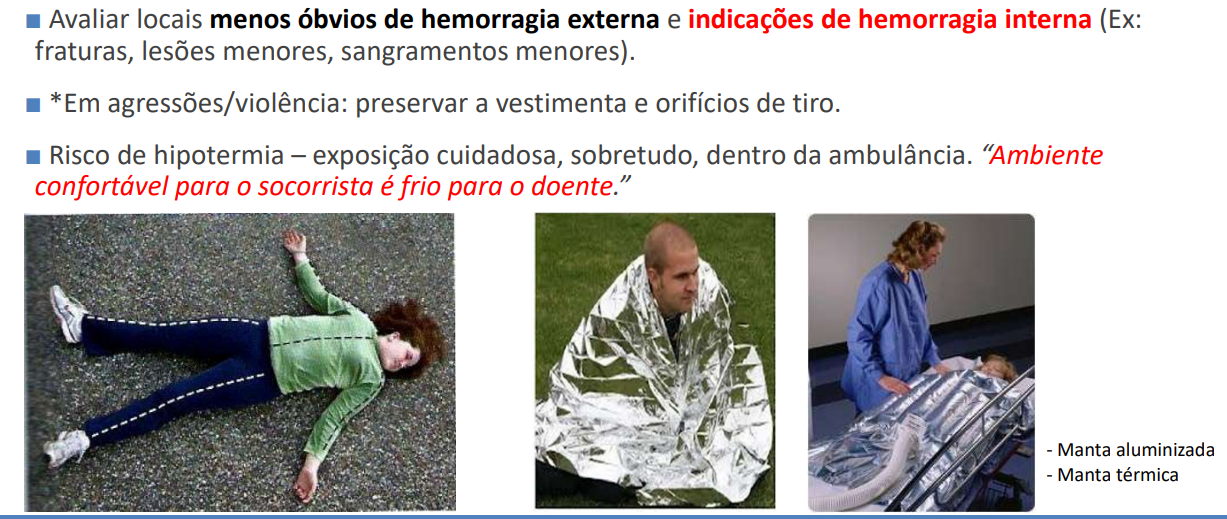
E – Exposure and Environmental Control
Secondary Assessment
The secondary assessment consists of history and head-to-toe physical exam looking for less severe problems. This phase should not be performed if there are changes in XABCDE-F — first, control life-threatening conditions.
If during the exam the patient deteriorates, immediately return to the primary exam.
Do not waste time at the scene with the secondary assessment! Perform it during transport to the hospital.
MOVE Protocol
- Monitor: level of consciousness, vital signs, TPR-BP every 3-5 minutes or when clinical change occurs
- Oxygen: maintain SpO₂ between 92-98%
- Vein: obtain 2 large-bore accesses
- Exams: electrocardiogram, capnography, blood gas analysis, gastric and urinary catheterization, AP chest X-ray, FAST ultrasound
History (SAMPLE)
- S – Symptoms/complaints
- A – Allergies to medications
- M – Medications in use
- P – Past medical and surgical history
- L – Last oral intake (liquids and foods)
- E – Event leading to trauma (biomechanics)
Perform the complete physical exam in cephalocaudal sequence, paying attention to the affected anatomical region.
Conclusion
The primary assessment aims to identify life-threatening conditions — respiratory, circulatory, and neurological. Understand the limitations of scene care and remember: your main objective is to safely and quickly transport the patient to definitive treatment.