What is Trauma and Why is it Not an Accident?
Trauma is not an "accident" in the sense of something inevitable. The word comes from Greek and means "wound" – an injury of variable extent, intensity, and severity, produced by physical, chemical, or electrical agents, whether intentional or not. Trauma is a preventable event, resulting from lack of care, attention, or ignorance.
As nurses, our role goes beyond immediate care. We need to understand trauma biomechanics – the study of forces acting on the body and how they generate injuries. This knowledge allows us to predict up to 90% of injuries before even touching the patient, guiding assessment and treatment.
PHTLS (Pre-Hospital Trauma Life Support) is the foundation for critical thinking in prehospital care. It is not a robotic protocol but a tool that develops decision-making skills for the most appropriate management in each scenario.
The Three Pillars of Trauma Care
Trauma care for the polytrauma patient is divided into three epidemiological stages:
- Pre-event: Prevention – seat belt use, helmets, traffic laws, education.
- Event: The moment of trauma – scene safety, response time, safe removal.
- Post-event: The "Golden Hour" – the first hour after trauma is crucial for survival. Ideal response time is 6 to 8 minutes, with up to 15 minutes on scene.
Steps of Care
- Scene assessment: Safety first. The rescuer is the most important person on site. Identify risks such as fire, electrical wires, traffic, aggressors, and hazardous materials.
- Biomechanics assessment: Understand what happened and how the patient was injured. This guides the search for hidden injuries.
- Primary survey (XABCDE): Airway, breathing, circulation, exposure.
- Secondary survey: History (SAMPLE) and detailed physical exam.
- Ongoing assessment: Continuous monitoring and reassessment.
Mechanisms of Injury: Blunt vs. Penetrating
Trauma can be blunt (closed) or penetrating (open). Each has specific mechanisms and injury patterns.
Blunt Trauma
Caused by compression and shearing. Examples: collisions, falls, run-overs.
- Frontal collisions: The body is projected upward or downward. Upward: skull fracture, cervical injury, brain contusion, aortic rupture (fatal in minutes), liver, spleen, and kidney injuries. Downward: ankle, femur, tibia fractures, knee and hip dislocation.
- Rear impact: Cervical hyperextension (whiplash) if the headrest is poorly positioned.
- Lateral impact: Clavicle fracture, rib fractures, pulmonary contusion, spleen injury (driver's side) or liver injury (passenger's side), pelvic fracture.
- Rollover: Multiple impacts, risk of ejection, shearing injuries to internal organs.
Falls: Considered severe when the height is 3 times the victim's height. Assess the impact surface and the body part that hit first. Don Juan Syndrome occurs when the feet hit the ground first, causing bilateral lower limb fractures.
Penetrating Trauma
Caused by permanent cavitation. Examples: stab wounds (SW) and gunshot wounds (GSW).
- SW: Regular, straight edges. In women, the movement is downward; in men, upward. Keep the weapon in place to assess trajectory.
- GSW: Oval/round edges, with possible abrasion area (gunpowder burn). The exit wound has a stellate appearance. Remember: 3 perforations may not mean 3 shots.
Cavitation, Shearing, and Compression
Three physical phenomena explain most injuries:
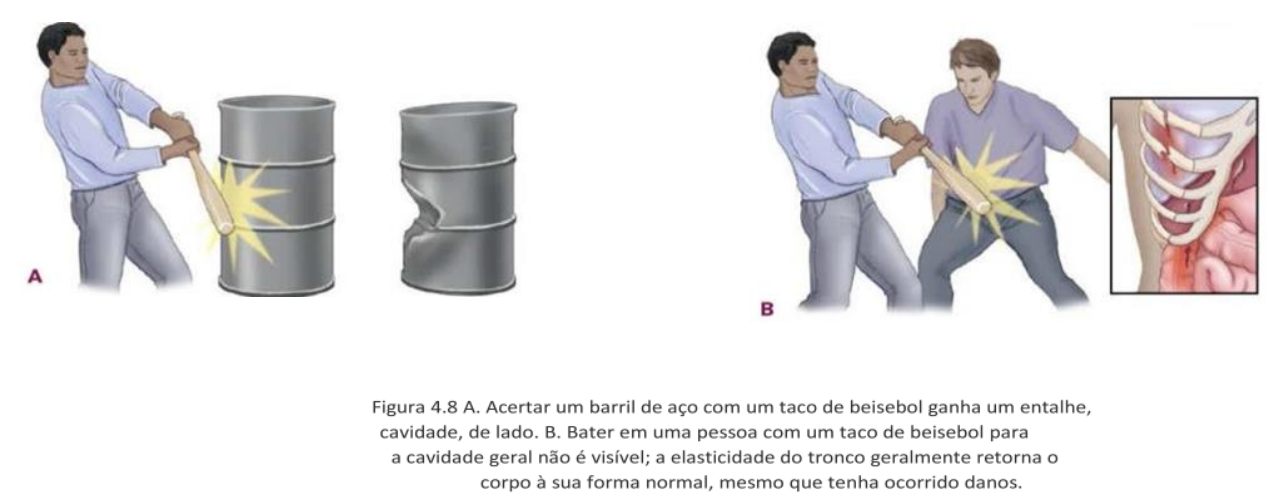
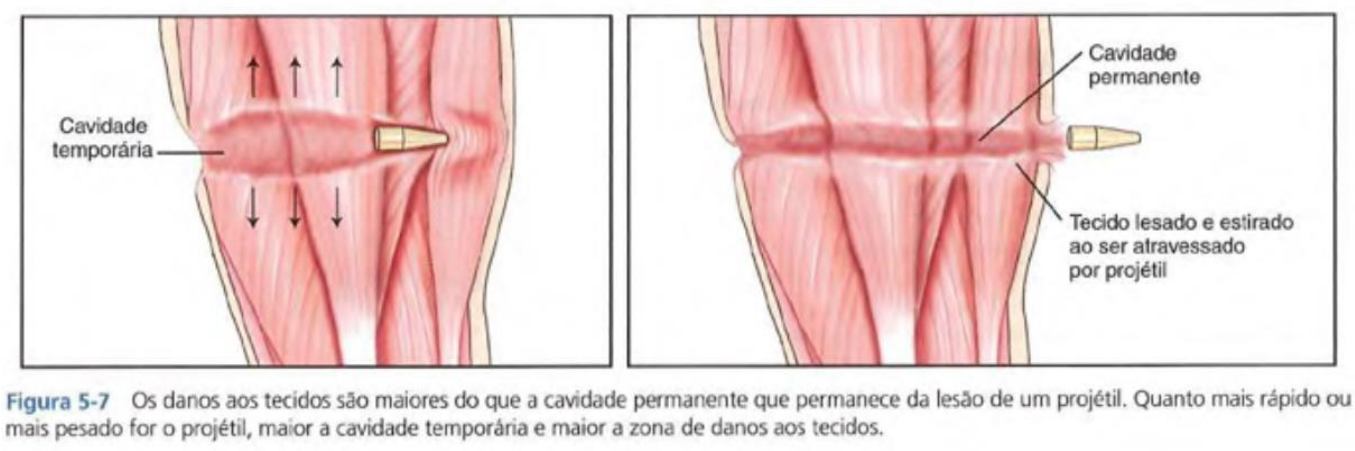
- Cavitation: When a solid object collides with the body, tissue particles are displaced, creating a cavity. It can be temporary (tissue returns to normal – blunt trauma) or permanent (tissue does not return – penetrating trauma).
- Shearing: An organ or structure changes speed faster than another, causing stretching injuries. Example: aortic rupture in frontal collisions.
- Compression: An organ or structure is compressed between others, like the liver between the sternum and spine.
Run-overs and Motorcycle Accidents
Run-overs have three phases:
- Vehicle impact with the pedestrian (adults: hips and legs; children: thorax/head).
- Torso rolls over the hood.
- Fall to the ground (head and cervical spine).
Motorcycle accidents: Frontal, angular impact, or ejection. The instinct to "lay the bike down" can cause asphalt burns.
Hemorrhage Control and Resuscitation
Control of significant external hemorrhage is a critical skill. Techniques include:
- Direct pressure with gauze or clean cloth.
- Elevation of the limb above the heart.
- Tourniquet (CAT or SWAT) when direct pressure fails.
- Hemostatic agents such as tranexamic acid.
Damage control resuscitation (DCR) in the prehospital setting involves aggressive hemorrhage control, permissive hypotension, and use of hemostatic agents to prevent exsanguination.
Conclusion
Understanding trauma biomechanics is essential for the emergency nurse. This knowledge allows:
- Assessing the need for additional resources.
- Increasing chances of survival.
- Identifying injuries more quickly.
- Initiating early treatment, reducing sequelae.
Stay updated with PHTLS guidelines and practice critical thinking. Every second counts – and knowledge saves lives.